U.S. rivers are getting into hot water. The frequency of river and stream heat waves is on the rise, a new analysis shows.
Like marine heat waves, riverine heat waves occur when water temperatures creep above their typical range for five or more days (SN: 2/1/22). Using 26 years of United States Geological Survey data, researchers compiled daily temperatures for 70 sites in rivers and streams across the United States, and then calculated how many days each site experienced a heat wave per year. From 1996 to 2021, the annual average number of heat wave days per river climbed from 11 to 25, the team reports October 3 in Limnology and Oceanography Letters.
The study is the first assessment of heat waves in rivers across the country, says Spencer Tassone, an ecosystem ecologist at the University of Virginia in Charlottesville. He and his colleagues tallied nearly 4,000 heat wave events — jumping from 82 in 1996 to 198 in 2021 — and amounting to over 35,000 heat wave days. The researchers found that the frequency of extreme heat increased at sites above reservoirs and in free-flowing conditions but not below reservoirs — possibly because dams release cooler water downstream.
Most heat waves with temperatures the highest above typical ranges occurred outside of summer months between December and April, pointing to warmer wintertime conditions, Tassone says.
Human-caused global warming plays a role in riverine heat waves, with heat waves partially tracking air temperatures — but other factors are probably also driving the trend. For example, less precipitation and lower water volume in rivers mean waterways warm up easier, the study says.
“These very short, extreme changes in water temperature can quickly push organisms past their thermal tolerance,” Tassone says. Compared with a gradual increase in temperature, sudden heat waves can have a greater impact on river-dwelling plants and animals, he says. Fish like salmon and trout are particularly sensitive to heat waves because the animals rely on cold water to get enough oxygen, regulate their body temperature and spawn correctly.
There are chemical consequences to the heat as well, says hydrologist Sujay Kaushal of the University of Maryland in College Park who was not involved with the study. Higher temperatures can speed up chemical reactions that contaminate water, in some cases contributing to toxic algal blooms (SN: 2/7/18).
The research can be used as a springboard to help mitigate heat waves in the future, Kaushal says, such as by increasing shade cover from trees or managing stormwater. In some rivers, beaver dams show promise for reducing water temperatures (SN: 8/9/22). “You can actually do something about this.”
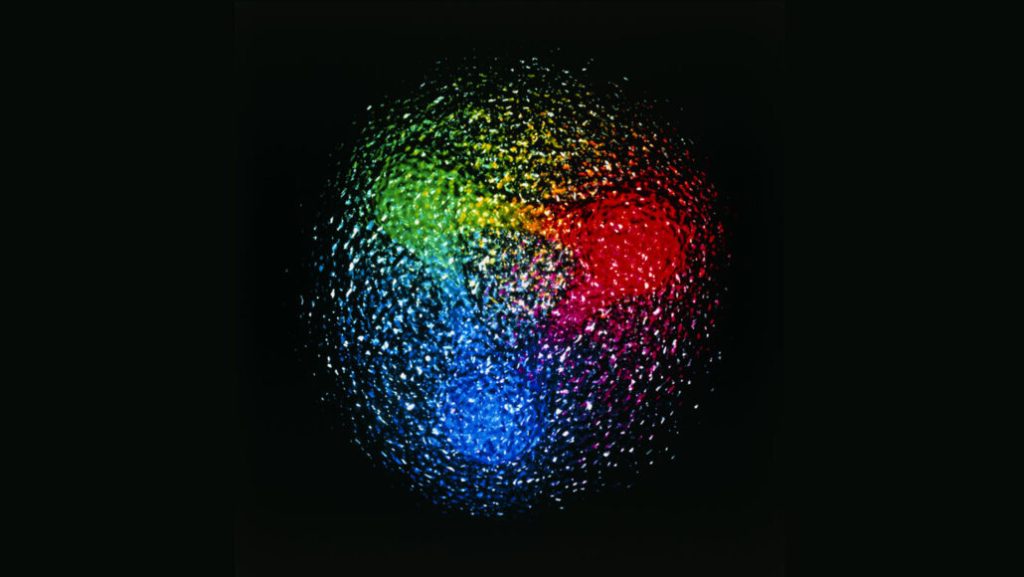
The subatomic particles are built of smaller particles called quarks, which are bound together by a powerful interaction known as the strong force. New experiments seem to show that the quarks respond more than expected to an electric field pulling on them, physicist Nikolaos Sparveris and colleagues report October 19 in Nature. The result suggests that the strong force isn’t quite as strong as theory predicts.
It’s a finding at odds with the standard model of particle physics, which describes the particles and forces that combine to make up us and everything around us. The result has some physicists stumped about how to explain it — or whether to even try. “It is certainly puzzling for the physics of the strong interaction, if this thing persists,” says Sparveris, of Temple University in Philadelphia.
Such stretchiness has turned up in other labs’ experiments, but wasn’t as convincing, Sparveris says. The stretchiness that he and his colleagues measured was less extreme than in previous experiments, but also came with less experimental uncertainty. That increases the researchers’ confidence that protons are indeed stretchier than theory says they should be.
At the Thomas Jefferson National Accelerator Facility in Newport News, Va., the team probed protons by firing electrons at a target of ultracold liquid hydrogen. Electrons scattering off protons in the hydrogen revealed how the protons’ quarks respond to electric fields (SN: 9/13/22). The higher the electron energy, the deeper the researchers could see into the protons, and the more the electrons revealed about how the strong force works inside protons.
For the most part, the quarks moved as expected when electric interactions pulled the particles in opposite directions. But at one point, as the electron energy was ramped up, the quarks appeared to respond more strongly to an electric field than theory predicted they would.
But it only happened for a small range of electron energies, leading to a bump in a plot of the proton’s stretch.
“Usually, behaviors of these things are quite, let’s say, smooth and there are no bumps,” says physicist Vladimir Pascalutsa of the Johannes Gutenberg University Mainz in Germany.
Pascalutsa says he’s often eager to dive into puzzling problems, but the odd stretchiness of protons is too sketchy for him to put pencil to paper at this time. “You need to be very, very inventive to come up with a whole framework which somehow finds you a new effect” to explain the bump, he says. “I don’t want to kill the buzz, but yeah, I’m quite skeptical as a theorist that this thing is going to stay.”
It will take more experiments to get theorists like him excited about unusually stretchy protons, Pascalutsa says. He could get his wish if Sparveris’ hopes are fulfilled to try the experiment again with positrons, the antimatter version of electrons, scattered from protons instead.
A different type of experiment altogether might make stretchy protons more compelling, Pascalutsa says. A forthcoming study from the Paul Scherrer Institute in Villigen, Switzerland, could do the trick. It will use hydrogen atoms that have muons in place of the electrons that usually orbit atoms’ nuclei. Muons are about 200 times as heavy as electrons, and orbit much closer to the nucleus of an atom than do electrons — offering a closer look at the proton inside (SN: 10/5/17). The experiment would involve stimulating the “muonic hydrogen” with lasers rather than scattering other electrons or positrons from them.
“The precision in the muonic hydrogen experiments will be much higher than whatever can be achieved in scattering experiments,” Pascalutsa says. If the stretchiness turns up there as well, “then I would start to look at this right away.”
You may have heard the big long COVID news that came out recently: A Scottish study reported that about half of people infected with SARS-CoV-2 have not fully recovered six to 18 months after infection. That result echoes what many doctors and patients have been saying for months. Long COVID is a serious problem and a huge number of people are dealing with it.
But it’s tough to find treatments for a disease that is still so ill-defined (SN: 7/29/22). One major research effort in the United States hopes to change that. And one of my colleagues, Science News’ News Director Macon Morehouse, got a peek into the process. In the last two months, Morehouse has donated 15 vials of blood, two urine specimens and a sample of saliva. Technicians have measured her blood pressure, oxygen level, height, weight and waist circumference and counted how many times she could rise from sitting to standing in 30 seconds. Morehouse is not sick, nor is she collecting data for her health. She’s doing it for science.
Morehouse is participating in a long COVID study at Howard University in Washington D.C. It’s part of a many-armed giant of a project with an eye on one thing: the long-term health effects of COVID-19. Launched last year by the National Institutes of Health, the RECOVER Initiative aims to enroll roughly 60,000 adults and children. At the Howard site, Morehouse is volunteer No. 182.
She’s somewhat of a unicorn among study participants: As far as she knows, Morehouse has never had COVID-19. Ultimately, some 10 percent of participants will include people who have avoided the virus, says Stuart Katz, a cardiologist and a RECOVER study leader at NYU Langone Health in New York City. Scientists continue to sign up volunteers, but “omicron made it harder to find uninfected people,” he says.
RECOVER scientists need participants like Morehouse so the researchers can compare them with people who developed long COVID. That might reveal what the disease is — and who it tends to strike. “Our goals are to define long COVID and to understand what’s your risk of getting [it] after COVID infection,” Katz says. Their results could be a first step toward developing treatments.
Tight timeline Within the pandemic’s first year, doctors noticed that some COVID-19 patients developed long-term symptoms such as brain fog, fatigue and chronic cough. In December 2020, Katz and other physicians and scientists convened to discuss what was known. The answer, it turned out, was not much. “This is a novel virus,” he says. “Nobody knew what it could do.” Around the same time, Congress OK’d $1.15 billion for the NIH to study COVID-19’s long-term health consequences.
Fast forward five months, and the agency had awarded nearly $470 million to NYU Langone Health to serve as the hub for its long COVID studies. “The whole thing was on a very, very compressed timeline,” Katz says. NYU then hustled to come up with a study plan focused on three main groups: adults, children/families and finally, tissue samples from people who died after having COVID-19. It wasn’t your typical research project, Katz says. “We were charged with studying a disease that didn’t have a definition.”
Today, RECOVER has enrolled just over half of a target 17,680 adults. Katz hopes to cross this finish line by spring 2023. The child-focused part of the project has further to go. The goal is to enroll nearly 20,000 children; so far, they’ve got around 1,200, says Diana Bianchi, director of the Eunice Kennedy Shriver National Institute of Child Health and Human Development and a member of RECOVER’s executive committee. Some scientists and patients have criticized RECOVER for moving too slowly. As someone who has recovered from long COVID himself, Katz says he gets it. “We started a year and a half ago, and we don’t yet have definitive answers,” he says. “For people that have been suffering, I can understand how it’s disappointing.”
But for RECOVER — with more than 400 doctors, scientists and other experts involved, roughly 180 sites across the country enrolling participants and a grant timeline that scuttled the usual order of events — the old saying about building the plane while flying it fits, Katz says. “We are working very, very hard to move as quickly as we can.”
Looking for answers Recently, other facets of the initiative have started to shine. An analysis of electronic health records found that among people under 21, kids younger than 5, kids with certain medical conditions and those who had had severe COVID-19 infections may be most at risk for long COVID, scientists reported in JAMA Pediatrics in August. And a different health records study suggests that vaccinated adults have some protection against long COVID, even if they had a breakthrough infection. Scientists posted that finding this month at medRxiv.org in a study that has yet to be peer-reviewed.
These studies tap data that have already been collected. The bulk of the RECOVER studies will take longer, because scientists will follow patients for years, analyzing data along the way. “These are observational, longitudinal studies,” Katz says. “There’s no intervention; we’re basically just trying to understand what long COVID is.”
Still, Katz expects to see early results later this fall. By then, scientists should have an official, if rough, definition of long COVID, which could help doctors struggling to diagnose the disease. By the end of the year, Katz says RECOVER might also have answers about viral persistence — whether coronavirus relics left behind in the body somehow reboot symptoms.
The project has also recently sprouted a clinical trials arm, which may launch this winter, says Kanecia Zimmerman, a pediatric critical care specialist who is leading this effort at the Duke Clinical Research Institute in North Carolina. One of the first trials planned will test whether an antiviral therapy that clears SARS-CoV-2 from the body helps patients with persistent symptoms.
Though RECOVER is a major effort to understand long COVID, progress will require research — and ideas — from a broad group of scientists, says Diane Griffin, a microbiologist at the Johns Hopkins Bloomberg School of Public Health in Baltimore and member of the Long COVID Research Initiative, who is not involved in the project. “Just because we’ve invested in this one big study, that’s not going to give us all the answers,” she says.
But information from study participants like Morehouse and the nearly 10,000 other adults who’ve already enrolled in RECOVER will help. In the meantime, continued support for long COVID research is crucial, Griffin says. “That’s the only way we’re going to eventually figure this out.”
In the summer of 1960, doctors extracted “crimson sludge” from 6-year-old Barbara Lowry’s bones and gave it to her twin.
That surgery, one of the first successful bone marrow transplants, belied the difficulty of the procedure. In the early years of transplantation, scores of patients died as doctors struggled to figure out how to use one person’s cells to treat another. “Cell therapy for blood diseases had a terrifying birth,” Siddhartha Mukherjee writes in his new book, The Song of the Cell.
The transplant story is one of many Mukherjee uses to put human faces and experiences at the heart of medical progress. But what radiates off the pages is the author himself. An oncologist, researcher and Pulitzer Prize–winning author, Mukherjee’s curiosity and wisdom add pep to what, in less dexterous hands, might be dry material. He finds wonder in every facet of cell biology, inspiration in the people working in this field and “spine-tingling awe” in their discoveries. It’s no surprise that Mukherjee is so seduced by science. This is a man who built a microscope from scratch during the pandemic and has spent years probing biology and its history with luminaries in the field. The Song of the Cell lets readers eavesdrop on these conversations, which can be intimate and enlightening.
On a car ride across the Netherlands, Mukherjee chats with geneticist Paul Nurse, who tells him about the cell division work that ultimately netted Nurse a Nobel Prize (SN: 3/27/21, p. 28). On a walk at Rockefeller University in New York
City, Mukherjee discusses his depression with another Nobel Prize–winning researcher, neuroscientist Paul Greengard. Mukherjee’s vivid imagery lends heft to his feelings. He tells Greengard about experiencing a “soupy fog of grief” after his father’s death and describes “drowning in a tide of sadness.”
In these memories, which Mukherjee uses to segue into the science of depression, and elsewhere in the book, hints of poetry shimmer among the prose. A cell observed under a microscope is “refulgent, glimmering, alive.” A white blood cell’s slow creep is like the “ectoplasmic movement of an alien.” Mukherjee weaves his experiences into the story of cell biology, guiding readers through the lives and discoveries of key figures in the field. We meet the “father of microbiology,” Antonie van Leeuwenhoek, a 17th century cloth merchant who ground globules of Venetian glass into microscope lenses and spied a “marvelous cosmos of a living world” within a raindrop. Mukherjee also teleports us to the present to introduce He Jiankui, the disgraced biophysicist behind the world’s first gene-edited babies (SN: 12/22/18 & 1/5/19, p. 20). Along the way, we also meet Frances Kelsey, the Food and Drug Administration medical officer who refused to approve thalidomide, a drug now known to cause birth defects, for use in the United States, and Lynn Margulis, the evolutionary biologist who argued that mitochondria and other organelles were once free-living bacteria (SN: 8/8/15, p. 22).
Mukherjee traverses a vast landscape of cell biology, and he’s not afraid to pull over and go exploring in the weeds. He describes in detail the flux of ions in nerve cells and introduces a considerable cast of immune system characters. For an even deeper dive, readers can check the footnotes; they are abundant.
What stands out most, though, are Mukherjee’s stories about people: scientists, doctors, patients and himself. As a researcher and a physician, he steps deftly between the scientific and clinical worlds, and, like the microscope he assembled, offers a glimpse into a universe we might not otherwise see.
Mountain lions have no interest in people, or the built-up areas we enjoy. But after a 2018 wildfire in California, local lions took more risks, crossing roads more often and moving around more in the daytime, scientists report October 20 in Current Biology. It’s another way the effects of human development could be putting pressure on vulnerable wildlife — in this case, potentially pushing them toward our bumpers.
The Woolsey Fire began near Los Angeles on November 8, 2018, and burned more than 36,000 hectares in the Santa Monica Mountains. Nearly 300,000 people evacuated, and three people died. Animals fled the fire too, including the local mountain lions (Puma concolor). The fire was a tragedy, but also a scientific opportunity, says Rachel Blakey, a global change biologist at UCLA. Many of the lions wore tracking collars, allowing scientists to study how the fire changed their behavior. Of the 11 collared cougars in the area at the time, nine made it to safety during the fire itself. “They have really large home ranges, so it’s nothing to them to be able to cover many kilometers in a day,” Blakey says.
No matter how much they moved, the mountain lions avoided people. One collared cat, P-64, initially fled the fire — until he got close to a developed area. Given the choice between fire and people, the lion retreated back into the burning area. “That’s where his movements stopped,” Blakey says. The park service later found P-64’s remains. He’d burned his paws, and it’s possible that he was unable to hunt and starved to death.
Using data from the nine lions that survived the fire and others collared after, the scientists showed that the cats generally avoided the severely burned areas of their territories. With vegetation gone, the cats had little cover for stalking and ambushing prey.
Instead, the cougars stuck to unburned areas, and continued to avoid people. But they took more risks around human infrastructure, increasing their road crossings from an average of about three times per month to five. These weren’t all two-lane country highways. The first collared lion to successfully cross Interstate 405, which has 10 lanes in places, did it after the Woolsey Fire. And the big cats crossed U.S. Route 101 once every four months, whereas before the fire, they’d crossed only once every two years. Their territories also overlapped more often, increasing the potential for deadly encounters between the solitary cats. And the generally nocturnal animals increased activity during daytime hours from 10 percent to 16 percent of their active time — boosting a lion’s chances of potentially bump into a human.
Road crossing is what Blakey calls a “risk mismatch.” Lions in areas with lots of people appear to weigh the risk of encountering humans as more dangerous. But “running across a freeway is a lot more likely to be fatal,” she says. That risk, combined with the risk of running into other cats, can be deadly. One young, collared male ended up dead on a freeway in the months after the fire. He was fleeing a fight with an older, uncollared male.
Intense burns like the Woolsey Fire highlight the resilience of mountain lions, says Winston Vickers, a wildlife research veterinarian at the University of California, Davis who was not involved in the study. “They have amazing mobility, they mostly can get away from the immediate fire, they mostly survive,” he notes. The changes in risk-taking, he says, could reflect how confined the population is, hemmed into the mountains by human development.
Wildlife crossings, such as the new Wallis Annenberg Wildlife Crossing over the 101, will hopefully give the mountain lions a safer option for roaming, though the main goal is to promote gene flow between lion populations, Blakey says (SN: 5/31/16). In a landscape where fire, humans and highways combine, it’s good to have somewhere to run.
What’s the matter? The proposed Windchime experiment plans to use only gravity to detect some types of dark matter. Ultrasensitive sensors would be jostled by the gravitational forces of a dark matter “wind” passing by Earth, James R. Riordon reported in “Gravity could aid dark matter search” (SN: 9/10/22, p. 14).
Since dark matter is affected by gravity, reader David Goldberg asked if dark matter orbits the Milky Way’s center just like our solar system does. If the two move together, how would there be a dark matter wind to detect?
It’s possible that dark matter circles the Milky Way’s center at least a little, though it’s hard to say for sure because no one has been able to measure the elusive stuff yet, Riordon says. But to search for dark matter using the Windchime method, it doesn’t really matter whether the mysterious substance moves with the galaxy, he says. That’s because as the sun circles the Milky Way’s center, Earth is also orbiting the sun. Even if the sun happens to move with the same velocity as nearby dark matter, the direction of Earth’s velocity changes over the course of a year, Riordon says. So we should sense the pull of a dark matter wind that shifts with Earth’s seasons.
What’s more, as the planet spins on its axis, the direction of the surface’s movement relative to the galaxy changes throughout the day. “It’s a little like a fish swimming in the ocean,” Riordon says. “Even though the water in general moves with Earth, as a fish swims in various directions, the creature will experience a flow of water relative to its own motion.”
Reader Jack Ryan wondered why, despite its gravitational attraction, dark matter doesn’t form stars, planets and other celestial bodies.
“Because no one knows what dark matter is, we can’t say for certain that it can or cannot form globs or come in very massive particles,” Riordon says. “It’s something that researchers like those on the Windchime team are looking out for.”
For normal matter to create asteroids or planets, it must experience some force beyond gravity, Riordon says. For instance, if two rocks collide in space, electromagnetic forces would prevent them from simply passing through each other. This would then allow gravity to hold the two rocks together. And if the concentration of matter continues to build up, then an asteroid or a planet could eventually form.
Some physicists hope that dark matter experiences other forces, but gravity is currently the only one known to affect it. “If a dark matter particle that only experiences gravity approaches a rock, a planet or another dark matter particle, it would glide right through because there is no force that can stop it,” Riordon says. “Gravity can pull dark matter into a halo, but on its own, it probably can’t stick dark matter together.” Correction A line dropped from our feature “Island lessons” (SN: 9/24/22, p. 22). At the end of Page 26, the full sentence should have read: Saban native Dahlia Hassell-Knijff got a degree in biology in Mississippi, then returned to the island, where she oversees projects at the regional Dutch Caribbean Nature Alliance.
In the fall of 2020, the world was staggering under the attack of the SARS-CoV-2 virus. In the United States, more than 4 million cases were reported in November, more than double the number in October. Hospitals were overwhelmed. On the Thursday before Thanksgiving, 1,962 people died.
Now, despite more than 1 million deaths in the United States and more than 6 million worldwide, it’s almost easy to forget that the pandemic’s assault continues. That is, until you hear Belinda Hankins’ story.
Hankins has been diagnosed with long COVID, a collection of symptoms that can include crushing fatigue, brain fog, pain and dizziness and that may affect 1 in 5 people infected with SARS-CoV-2, according to one conservative estimate. She talked with Science News staff writer Meghan Rosen during her appointment at the long COVID clinic at the Johns Hopkins Bayview Medical Center.
“For months we’ve heard estimates about how many people have long COVID,” Rosen told me. “I was interested in going beyond the stats to find out what it’s like for the patients and doctors living with this.”
That effort involved talking with doctors who are trying to figure out how to treat the symptoms of long COVID when the cause is still unknown. And talking with Hankins. “I thought it was extraordinary that [she] let me into her appointment,” Rosen said. “It’s just so generous and so brave.”
I share Rosen’s gratitude. Asking someone in the midst of a life-altering illness to talk with a journalist is a big request. I always worry that people might feel pressure to participate, and I want to be sure that they’ve had time to think through the implications of going public with personal information. Hankins was clear about why she said yes. “She wanted to share her story because a lot of people in her life don’t know what long COVID is and why she’s still so sick,” Rosen said.
In reporting, Rosen brings both her empathy and her serious science chops. She has a Ph.D. in biochemistry and molecular biology and is a graduate of the science journalism program at the University of California, Santa Cruz. She explored careers in biotech but decided that wasn’t the right fit. She wanted to write about health and medicine.
This is actually Rosen’s third stint at Science News: first as an intern, then as a reporter, and now back on the beat after five years of doing communications work for the Howard Hughes Medical Institute. We’re glad she’s back. Not only is she tackling complex issues surrounding COVID-19, including how U.S. public health guidelines affect kids in school (SN Online: 8/19/22), she’s also been sharing her delight in science. That includes stories on genetic variants linked to uncombable hair in children (SN: 10/8/22 & 10/22/22, p. 5); an unusual “snough” call that zoo gorillas appear to have invented to get zookeepers’ attention (SN Online: 8/10/22); and a new robotic pill designed to deliver drugs by scrubbing away mucus in the intestines.
Yes, science is serious and important, but it’s also crazy fun. I don’t think I’m ready to sign up for the robotic intestinal scrub brush, but I sure do enjoy finding out about it.
Across the United States, kids are prepping for back-to-school, or are already in classrooms, and parents are buckling up for another pandemic school year. Like me, many are trying to get a handle on what COVID-19 precautions to take. Updated guidance released last week by the U.S. Centers for Disease Control and Prevention hasn’t exactly helped. It may have made dealing with back-to-school more confusing — and could even spur new outbreaks.
Last November, my fifth grader had to quarantine at home for 10 days after a close contact tested positive. Now, the CDC has nixed the quarantine recommendation for people exposed to COVID-19. Today, our situation could look something like this: My COVID-exposed daughter would mask for 10 days, test on day five, and remain in school the whole time — only the infected child would isolate. That child would stay home for at least five days after a positive test. Then, if the child is fever-free and symptoms are improving, according to the new guidance, they could pop on a mask and hightail it back to class — no testing needed. That advice could mean more COVID-19 in classrooms. Scientists have shown that people can remain infectious after day five. So without testing for COVID-19, students and teachers won’t know if they’re bringing the disease back to school.
On the same day the CDC’s guidance came out, the U.S. Food and Drug Administration added yet another wrinkle. If you think you’ve been exposed to COVID-19 but test negative with an at-home COVID-19 antigen test, the FDA now recommends testing again … and again. Repeat testing over time cuts the chances you’ll miss an infection and unknowingly spread the virus, the FDA advised on August 11.
It’s hard to say how that advice jibes with the CDC’s new, more-relaxed guidelines. Even the agency has said its public guidance during the pandemic has been “confusing and overwhelming,” the New York Times reports. CDC director Rochelle Walensky is now planning a shake-up that could include restructuring the communications office as well as relying more on preliminary studies rather tha The CDC’s new guidance has sparked a range of reactions, many negative, among scientists, doctors, parents and teachers. In an informal Twitter poll of Science News followers, roughly 80 percent of the 353 respondents reported that the new CDC guidance made them feel confused, worried or angry and/or exasperated.
Now, it’s up to local school districts to decide what COVID-19 measures to take. “Just because guidance has changed does not mean COVID is gone,” Becky Pringle, president of the National Education Association labor union, said in a statement. Not by a long shot. The United States is currently averaging nearly 500 daily coronavirus deaths and more than 100,000 new cases a day, an almost certain undercount.
As my own children gear up for school, I wonder about COVID-19’s constantly shifting landscape. Like other families with school-aged children, we’ve bounced from virtual school to in-person mask mandates to mask-optional recommendations. And we still don’t know our district’s plans for the upcoming year. School starts in about a week.
There is reason for hope, though: We know what measures can slow COVID-19’s spread in schools. Masking is a big one. A preliminary study posted August 9 linked lifting school mask mandates in Boston-area K–12 schools with a rise in cases among students and staff. At Boston University, mandatory masking plus a vaccine mandate seemed to keep the virus in check in classrooms, scientists reported August 5 in JAMA Network Open. Testing can help, too. A computer analysis from England suggests that regularly rapid testing students can curb classroom transmission, scientists report August 10 in the Royal Society Open Science. But knowing what works is not the same as actually employing evidence-based measures in the classroom, says Anne Sosin, a public health researcher at Dartmouth College whose research focuses on COVID-19 and rural health equity. She has studied how pandemic policies have impacted schools in northern New England. “I worry that we simply have not seen the political leadership to ensure that all children and educators can safely participate in school.”
I spoke with Sosin about the CDC’s new guidance, and what kids and parents might expect heading into the new school year. Our conversation has been edited for length and clarity.
SN: What do you think of the updated guidance?
Sosin: I was very disappointed that the CDC did not adopt a test-to-exit-isolation recommendation.
What we’re going to see in schools are infected students and educators returning after five days still positive for COVID-19. Multiple studies have demonstrated that most people are infectious beyond five days. Not only is it highly likely that they’ll be seeding outbreaks. They’ll also be putting high-risk members of school communities in danger.
SN: What could the guidance mean for vulnerable kids?
Sosin: I think that vulnerable people are going to be in a very precarious situation. The guidance mentions the need to ensure protections for immunocompromised and other high-risk people but there’s a problem of implementation. Will schools actually implement those protections?
SN: Do scientists have a good handle on what protections can help?
Sosin: Definitely. We have really strong evidence showing that when layered mitigation strategies are in place, we can almost eliminate transmission in school settings. That means that we should have upgraded ventilation, lunchroom strategies [like taking kids outside to eat] and testing. And I continue to think that data-driven mask policies have a role to play. Not masking forever, but masking at times when we see an uptick in transmission.
SN: How could the new guidance affect different communities across the United States?
Sosin: Different communities have not only been impacted in dramatically different ways, but they’re also on unequal footing at this stage of the pandemic.
[If we compare white communities with communities of color], we see disparities in vaccination coverage and caregiver loss. Some communities have suffered enormous losses while others have really been untouched. Black children have lost caregivers at more than two times the rate of white children. For Indigenous children, the rate is 4.5 times as high. Those are sharp disparities.
Communities of color also have less access to testing, treatment and health care. I worry that if we don’t have a renewed focus on equity, then we’re just going to see an exacerbation of disparities that have existed throughout the pandemic.
SN: What advice do you have for parents as they head into the new school year?
Sosin: We all want as normal a school year as possible. Masking should be one of the tools we’re ready to employ to keep our kids in the classroom. In addition, we should be advocating that our schools invest in ventilation. Vaccination also represents a critical piece of the strategy.
We see such abysmal vaccination coverage among children. Less than 1 in 3 kids ages 5 to 11 are fully vaccinated. I think many parents no longer see it as important — there’s been this narrative that the pandemic is over. We need clear messaging that vaccination remains an important tool.
Now is a great time to plan back-to-school campaigns to vaccinate kids and to begin to prepare for the arrival of omicron-specific boosters in the fall.
Archaeologist Peter Bellwood’s academic odyssey wended from England to teaching posts halfway around the world, first in New Zealand and then in Australia. For more than 50 years, he has studied how humans settled islands from Southeast Asia to Polynesia.
So it’s fitting that his new book, a plain-English summary of what’s known and what’s not about the evolution of humans and our ancestors, emphasizes movement. In The Five-Million-Year Odyssey, Bellwood examines a parade of species in the human evolutionary family — he collectively refers to them as hominins, whereas some others (including Science News) use the term hominids (SN: 9/15/21) — and tracks their migrations across land and sea. He marshals evidence indicating that hominids in motion continually shifted the direction of biological and cultural evolution. Throughout his tour, Bellwood presents his own take on contested topics. But when available evidence leaves a debate unresolved, he says so. Consider the earliest hominids. Species from at least 4.4 million years ago or more whose hominid status is controversial, such as Ardipithecus ramidus, get a brief mention. Bellwood renders no verdict on whether those finds come from early hominids or ancient apes. He focuses instead on African australopithecines, a set of upright but partly apelike species thought to have included populations that evolved into members of our own genus, Homo, around 2.5 million to 3 million years ago. Bellwood hammers home the point that stone-tool making by the last australopithecines, the first Homo groups or both contributed to the evolution of bigger brains in our ancestors.
The action speeds up when Homo erectus becomes the first known hominid to leave Africa, roughly 2 million years ago. Questions remain, Bellwood writes, about how many such migrations occurred and whether this humanlike species reached distant islands such as Flores in Indonesia, perhaps giving rise to small hominids called hobbits, or Homo floresiensis (SN: 3/30/16). What’s clear is that H. erectus groups journeyed across mainland Asia and at least as far as the Indonesian island of Java.
Intercontinental migrations flourished after Homo sapiens debuted, around 300,000 years ago in Africa. Bellwood regards H. sapiens, Neandertals and Denisovans as distinct species that interbred in certain parts of Asia and Europe. He suggests that Neandertals disappeared around 40,000 years ago as they mated with members of more numerous H. sapiens populations, leaving a genetic legacy in people today. But he does not address an opposing argument that different Homo populations at this time, including Neandertals, were too closely related to have been separate species and that it was intermittent mating among these mobile groups that drove the evolution of present-day humans (SN: 6/5/21).
Bellwood gives considerable attention to the rise of food production and domestication in Europe and Asia after around 9,000 years ago. He builds on an argument, derived from his 2004 book First Farmers, that expanding populations of early cultivators migrated to new lands in such great numbers that they spread major language families with them. For instance, farmers in what’s now Turkey spread Indo-European languages into much of Europe sometime after roughly 8,000 years ago, Bellwood contends.
He rejects a recent alternative proposal, based on ancient DNA evidence, that horse-riding herders of Central Asia’s Yamnaya culture brought their traditions and Indo-European tongues to Europe around 5,000 years ago (SN: 11/15/17). Too few Yamnaya immigrated to impose a new language on European communities, Bellwood says. Similarly, he argues, ancient Eurasian conquerors, from Alexander the Great to Roman emperors, couldn’t get speakers of regional languages to adopt new ones spoken by their outnumbered military masters.
Bellwood rounds out his evolutionary odyssey with a reconstruction of how early agricultural populations expanded through East Asia and beyond, to Australia, a string of Pacific islands and the Americas. Between about 4,000 and 750 years ago, for instance, sea-faring farmers spread Austronesian languages from southern China and Taiwan to Madagascar in the west and Polynesia in the east. Precisely how they accomplished that remarkable feat remains a puzzle.
Disappointingly, Bellwood doesn’t weigh in on a recent archaeological argument that ancient societies were more flexible and complex than long assumed (SN: 11/9/21). On the plus side, his evolutionary odyssey moves along at a brisk pace and, like our ancestors, covers a lot of ground.
Sometimes a photo is literally a matter of life, death — and zombies.
This haunting image, winner of the 2022 BMC Ecology and Evolution photography competition, certainly fits that description. It captures the fruiting bodies of a parasitic fungus, emerging from the lifeless body of an infected fly in the Peruvian rainforest.
The fungus-infested fly was one of many images submitted to the contest from all over the world, aiming to showcase the beauty of the natural world and the challenges it faces. The journal revealed the winners August 18. Roberto García-Roa, a conservation photographer and evolutionary biologist at the University of Valencia in Spain, took the winning photo while visiting the Tambopata National Reserve, a protected habitat in the Amazon.
The fungus erupting from the fly belongs to the genus Ophiocordyceps, a diverse collection of parasitic fungi known as “zombie fungi,” due to their ability to infect insects and control their minds (SN: 7/17/19).
“There is still much to unravel about the diversity of these fungi as it is likely that each insect species infected succumbs to its own, specialized fungus,” says Charissa de Bekker, an expert in parasitic fungi at Utrecht University in the Netherlands.
First, spores of the fungus land on the ill-fated fly. So begins the manipulative endgame. The spores infiltrate the fly’s exoskeleton before infecting its body and eventually hijacking its mind. Once in control, the fungus uses its new powers of locomotion to relocate to a microclimate more suitable to its own growth — somewhere with the right temperature, light and moisture.
Fungus and fly then bide their time until the fly dies, becoming a food source for the fungus to consume. Fruiting bodies work their way out of the fly, filled with spores that are released into the air to continue the macabre cycle in a new, unsuspecting host. It is a “conquest shaped by thousands of years of evolution,” García-Roa said in a statement announcing the winners.
Research into the molecular aspects of fungal mind control is under way, De Bekker says, including in her own lab. “These fungi harbor all sorts of bioactive chemicals that we have yet to characterize and that could have novel medicinal and pest control applications.”