A crucial link in the life cycle of one parasitic plant may be found in a surprising place — the bellies of the descendants of an ancient line of rabbits.
Given their propensity for nibbling on gardens and darting across suburban lawns, it can be easy to forget that rabbits are wild animals. But a living reminder of their wildness can be found on two of Japan’s Ryukyu Islands, if you have the patience to look for it: the endangered Amami rabbit, a “living fossil” that looks strikingly similar to ancient Asian rabbits. One estimate suggests there are fewer than 5,000 of the animals left in the wild. The lives of Amamis (Pentalagus furnessi) are shrouded in mystery due to their rarity, but they seem to play a surprising ecological role as seed dispersers, researchers report January 23 in Ecology.
Seed dispersal is the main point in a plant’s life cycle when it can move to a new location (SN: 11/14/22). So dispersal is crucially important for understanding how plant populations are maintained and how species will respond to climate change, says Haldre Rogers, a biologist at Virginia Tech in Blacksburg, who was not involved with the study. Despite this, seed dispersal hasn’t received much attention, she says. “We don’t know what disperses the seeds of most plants in the world.”
Locals from the Ryukyu Islands were the first to notice that the “iconic yet endangered” Amami rabbit was nibbling on the fruit of another local species, the plant Balanophora yuwanensis, says Kenji Suetsugu, a biologist at Kobe University in Japan.
Rabbits generally like to eat vegetative tissue from plants, like leaves and stems, and so haven’t been thought to contribute much to spreading seeds, which are often housed in fleshy fruits.
To confirm what the locals reported, Suetsugu and graduate student Hiromu Hashiwaki set up camera traps around the island to catch the rabbits in the act. The researchers were able to record rabbits munching on Balanophora fruits 11 times, but still needed to check whether the seeds survived their trip through the bunny tummies. So the team headed out to the subtropical islands and scooped up rabbit poop, finding Balanophora seeds inside that could still be grown. By swallowing the seeds and pooping them out elsewhere, the Amami rabbits were clearly acting as seed dispersers.
Balanophora plants are parasitic and don’t have chlorophyll, so they can’t use photosynthesis to make food of their own (SN: 3/2/17). Instead, they suck energy away from a host plant. This means where their seeds end up matters, and the Amami rabbits “may facilitate the placement of seeds near the roots of a compatible host” by pooping in underground burrows, Suetsugu says. “Thus, the rabbits likely provide a crucial link between Balanophora and its hosts” that remains to be further explored, he says. Understanding the ecology of an endangered species like the Amami rabbit can help with conserving both it and the plants that depend on it.
An animal need not be in obvious peril for a change in its number to affect seed dispersal, with potentially negative consequences for the ecosystem. For example, “we think of robins as super common … but they’ve declined a lot in the last 50 years,” Rogers says. “Half as many robins means half as many seeds are getting moved around, even though no one’s worried about robins as a conservation issue.”
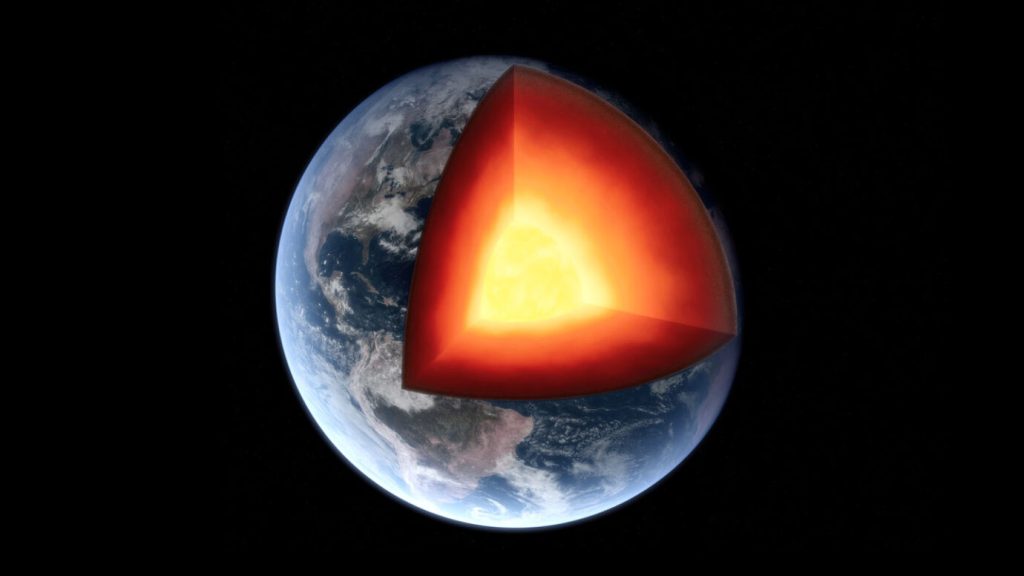
Earth’s inner core may have temporarily stopped rotating relative to the mantle and surface, researchers report in the January 23 Nature Geoscience. Now, the direction of the inner core’s rotation may be reversing — part of what could be a roughly 70-year-long cycle that may influence the length of Earth’s days and its magnetic field — though some researchers are skeptical.
“We see strong evidence that the inner core has been rotating faster than the surface, [but] by around 2009 it nearly stopped,” says geophysicist Xiaodong Song of Peking University in Beijing. “Now it is gradually mov[ing] in the opposite direction.” Such a profound turnaround might sound bizarre, but Earth is volatile (SN: 1/13/21). Bore through the ever-shifting crust and you’ll enter the titanic mantle, where behemoth masses of rock flow viscously over spans of millions of years, sometimes upwelling to excoriate the overlying crust (SN: 1/11/17, SN: 3/2/17, SN: 2/4/21). Delve deeper and you’ll reach Earth’s liquid outer core. Here, circulating currents of molten metals conjure our planet’s magnetic field (SN: 9/4/15). And at the heart of that melt, you’ll find a revolving, solid metal ball about 70 percent as wide as the moon.
This is the inner core (SN: 1/28/19). Studies have suggested that this solid heart may rotate within the liquid outer core, compelled by the outer core’s magnetic torque. Researchers have also argued the mantle’s immense gravitational pull may apply an erratic brake on the inner core’s rotation, causing it to oscillate.
Evidence for the inner core’s fluctuating rotation first emerged in 1996. Geophysicist Paul Richards of Columbia University’s Lamont-Doherty Earth Observatory in Palisades, N.Y., and Song, then also at Lamont-Doherty, reported that over a span of three decades, seismic waves from earthquakes took different amounts of time to traverse Earth’s solid heart.
The researchers inferred that the inner core rotates at a different speed than the mantle and crust, causing the time differences. The planet spins roughly 360 degrees in a day. Based on their calculations, the researchers estimated that the inner core, on average, rotates about 1 degree per year faster than the rest of Earth.
But other researchers have questioned that conclusion, some suggesting that the core spins slower than Song and Richards’ estimate or doesn’t spin differently at all.
In the new study, while analyzing global seismic data stretching back to the 1990s, Song and geophysicist Yi Yang — also at Peking University — made a surprising observation. Before 2009, seismic waves generated by sequences and pairs of repeating earthquakes — known as multiplets and doublets — traveled at different rates through the inner core. This indicated the waves from recurring quakes were crossing different parts of the inner core, and that the inner core was rotating at a different pace than the rest of Earth, aligning with Song’s previous research.
But around 2009, the differences in travel times vanished. That suggested the inner core had ceased rotating with respect to the mantle and crust, Yang says. After 2009, these differences returned, but the researchers inferred that the waves were crossing parts of the inner core that suggested it was now rotating in the opposite direction relative to the rest of Earth.
The researchers then pored over records of Alaskan earthquake doublets dating to 1964. While the inner core appeared to rotate steadily for most of that time, it seems to have made another reversal in rotation in the early 1970s, the researchers say.
Song and Yang infer that the inner core may oscillate with a roughly 70-year periodicity — switching directions every 35 years or so. Because the inner core is gravitationally linked to the mantle and magnetically linked to the outer core, the researchers say these oscillations could explain known 60- to 70-year variations in the length of Earth’s days and the behavior of the planet’s magnetic field. However, more work is needed to pin down what mechanisms might be responsible.
But not all researchers are on board. Yang and Song “identif[y] this recent 10-year period [that] has less activity than before, and I think that’s probably reliable,” says geophysicist John Vidale of the University of Southern California in Los Angeles, who was not involved in the research. But beyond that, Vidale says, things get contentious.
In 2022, he and a colleague reported that seismic waves from nuclear tests show the inner core may reverse its rotation every three years or so. Meanwhile, other researchers have proposed that the inner core isn’t moving at all. Instead, they say, changes to the shape of the inner core’s surface could explain the differences in wave travel times.
Future observations will probably help disentangle the discrepancies between these studies, Vidale says. For now, he’s unruffled by the purported chthonic standstill. “In all likelihood, it’s irrelevant to life on the surface, but we don’t actually know what’s happening,” he says. “It’s incumbent on us to figure it out.”
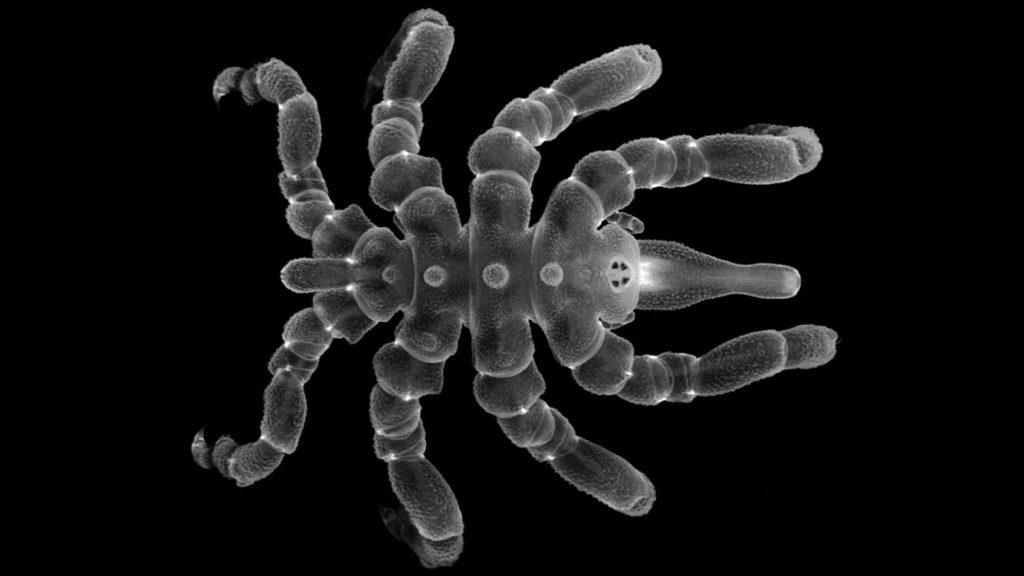
No backside, no problem for some young sea spiders.
The creatures can regenerate nearly complete parts of their bottom halves — including muscles, reproductive organs and the anus — or make do without them, researchers report January 23 in Proceedings of the National Academy of Sciences.
The ability to regrow body parts isn’t super common, but some species manage to pull it off. Some sea slug heads can craft an entirely new body (SN: 3/8/21). Sea spiders and some other arthropods — a group of invertebrates with an exoskeleton — can regrow parts of their legs. But researchers thought new legs were the extent of any arthropod’s powers, perhaps because tough exteriors somehow stop them from regenerating other body parts. A mishap first clued evolutionary biologist Georg Brenneis in that sea spiders (Pycnogonum litorale) might be able handle more complex repairs too. He accidentally injured one young specimen that he was working on in the lab with forceps. “It wasn’t dead, it was moving, so I just kept it,” says Brenneis, of the University of Vienna. Several months later, the sea spider had an extra leg instead of a scar, he and evolutionary biologist Gerhard Scholtz of Humbolt University of Berlin reported in 2016 in The Science of Nature.
In the new study, most of the 19 young spiders recovered and regrew missing muscles and other parts of their lower halves after amputation, though the regeneration wasn’t always perfect. Some juveniles sported six or seven legs instead of eight.
None of four adults regenerated. That may be because adults no longer shed their skin as they grow, suggesting that regeneration and molting are somehow linked, Brenneis says. Two young sea spiders also didn’t regenerate at all. The animals survived with only four legs and without an anus. Instead of pooping, the pair regurgitated waste out of their mouths. Next up is figuring out whether other arthropods also regenerate more than scientists thought, and how sea spiders do it, Brenneis says. “I would like to see how it works.”
A new smartwatch app alerts users who are deaf or hard of hearing of nearby sounds, such as microwave beeps or car horns.
“The main motivation [for the app] came from my own experience, and conversations that my colleagues and I have had with deaf and hard of hearing people over several years,” says Dhruv Jain, who presented the system, called SoundWatch, at the virtual ASSETS conference on October 28.
Jain, who is hard of hearing, uses SoundWatch at home to avoid sleeping through a smoke alarm. “On a nature walk, it’ll tell me that there’s birds chirping, or there might be a waterfall nearby,” he says. “Those sounds make me feel more present and connected to the world.”
Sound awareness apps for smartphones exist. But Jain prefers the immediacy of sound notifications on his wrist, rather than in his pocket — and surveys of people who are deaf or hard of hearing show he’s not alone.
The SoundWatch app pairs an Android smartwatch and phone. The watch records ambient noises and sends that data to the phone for processing. When the phone detects a sound of interest, the smartwatch vibrates and displays a notification.
Jain, a computer scientist at the University of Washington in Seattle, and colleagues designed the app to identify 20 noises. In experiments, SoundWatch correctly identified those 20 sounds 81.2 percent of the time. When set to listen only for urgent noises — a fire alarm, door knock or alarm clock — the app was 97.6 percent accurate. Eight deaf and hard of hearing people who used SoundWatch around a university campus gave the app broadly favorable reviews, but noted that the app misclassified some sounds in noisy outdoor settings.
Jain and colleagues are now working on a version of SoundWatch that users can train to recognize new sounds, such as their own house alarm, using just a few recordings.
November is beginning to feel a lot like last March.
In Europe, where the coronavirus was largely under control for much of the summer and fall, cases are skyrocketing nearly everywhere. Twenty countries, including the United Kingdom and France, have shuttered restaurants, introduced curfews or generally urged people to stay at home, though most schools and universities are staying open for now.
Cases are surging across the United States, too, where more than 100,000 new infections are being reported each day. Already in November, more than half of states have set records for the most cases in a week, and in places such as Minnesota, Utah and Wisconsin, some hospitals are nearing capacity. In North Dakota, nearly 1 in every 14 people has already contracted the coronavirus, with 2,254 cases reported November 8 alone in a state of 762,000 people.
To make matters worse, “the virus is going into its sweet spot at a time that we’re exhausted by it,” says Jeffrey Shaman, an infectious diseases epidemiologist at the Columbia University Mailman School of Public Health in New York City. That sweet spot is indoors, where people are spending more time as the weather in the Northern Hemisphere turns colder — and where the virus can spread more easily.
Despite such a grave outlook, experts say it’s still not too late to turn the tide.
Shutting down borders, businesses and schools are among the most drastic measures to do that. Worries over economic consequences may hold governments back from issuing widespread stay-at-home orders this time around, though.
U.S. President-elect Joe Biden, who unveiled a COVID-19 advisory board November 9, has proposed a multipronged plan for controlling the pandemic, including nationwide mask mandates and expanded testing. But Biden won’t take office until January 20, and President Donald Trump has repeatedly downplayed the surge in cases.
While getting a COVID-19 vaccine — or vaccines — is closer than ever (SN: 11/9/20), most experts agree that vaccines probably won’t be available to everybody until late spring or early summer. That means getting through the winter will require falling back on the familiar public health tools of physical distancing, mask wearing, and testing and isolating infected people, Shaman says. But all of those measures fall short unless everyone is willing to follow the rules.
Living in this reality can be draining, acknowledges Aleksandra Zając, a doctor specializing in nuclear medicine in Warsaw. Doctors and patients alike are tired of not being able to leave their homes and having to wear a mask when they do, she says, but “as a doctor, I really see the need for all those restrictions.” People aren’t helpless against the virus, she says. “We still have some impact on what’s going on.” Zając devised a calculator to help people learn how much wearing masks and goggles, regularly washing their hands and keeping distance from others might help protect them. Alone, none of those measures is perfect, but doing them all together can boost protection, like layering slices of Swiss cheese so that holes in one slice are covered by another slice. The Swiss cheese idea is not new, but it’s still relevant for stacking public health measures, Zając says. It goes for individual actions, too.
“One individual cannot do much” beyond protecting themselves, Zając says, “but if we sum up all the individuals together and they all follow the rules, I truly believe we can control this pandemic.”
Scientists know much more about the virus than they did in March, and that knowledge can help make the most of all the public health tools at our disposal.
Mask up Dozens of studies have made it abundantly clear that wearing a mask is one of the most effective steps an individual can take to help curb the pandemic. Masks are especially crucial in lessening the risk of someone who doesn’t know they’re infected passing the virus to someone else (SN: 6/26/20).
Additionally, there’s a growing understanding among scientists that masks are good for the wearer too. The U.S. Centers for Disease Control and Prevention updated their scientific guidance on November 10 to acknowledge that cloth masks can reduce the number of infectious droplets inhaled by the wearer, which offers a degree of protection, especially when masks are multi-layered.
In a study published October 23 in Nature Medicine, scientists estimate that if 95 percent of people wore masks when outside their homes, nearly 130,000 deaths from COVID-19 might be averted in the United States between the end of September and the end of February 2021. If 85 percent of people wear masks, about 96,000 lives might be saved, the researchers calculate.
The debate over which kind of mask is best, however, has been spirited (SN: 8/12/20).
When it comes to ubiquitous cloth masks, only one randomized clinical trial in the world is testing their effectiveness in preventing COVID-19. That trial in Guinea-Bissau is giving all 66,000 expected participants advice about how to avoid respiratory illnesses. Half of those people will each also get two locally sewn cloth masks. The trial is expected to wrap up in November.
Some research on the prevention of other respiratory illnesses suggests that a cloth mask’s effectiveness depends on many factors, including wearing the mask properly over both the nose and mouth. Regular washing in hot water is also necessary, says Raina MacIntyre, a mask researcher at the University of New South Wales in Sydney. In 2015, she and colleagues published in BMJ Open results of a trial conducted in Hanoi, Vietnam. Roughly 1,600 health care workers at 15 hospitals were assigned to either wear a medical mask at all times during their shift, to wear a two-layer cloth mask or to follow the hospital’s standard practice, which may or may not involve wearing a mask. The results weren’t encouraging. At the end of the five-week study, people in the cloth mask group had the highest rate of respiratory infections, such as colds — even higher than the group that wasn’t regularly wearing masks. The researchers concluded that health care workers shouldn’t wear cloth masks and opt instead for medical masks.
The trial was very controversial, MacIntyre says, “because the message was that cloth masks could be dangerous. That caused a lot of angst during the pandemic. In March and April, I had a lot of health workers in the U.S. and Europe contacting me and saying, ‘The hospital has run out of respirators. Is it better I wear no mask than wear a cloth mask?’”
That prompted MacIntyre and colleagues to examine unpublished data from the trial. Both surgical and cloth masks get contaminated with respiratory viruses, the researchers found. But surgical masks are disposable. If people didn’t wash their reusable cloth masks every day, the masks became more and more contaminated.
“If you washed your cloth mask in a washing machine with hot water, you were just as protected as wearing a surgical mask,” MacIntyre says. But workers who hand-washed their masks had double the risk of infection of those wearing a medical mask, the researchers reported September 28 in BMJ Open. “The bottom line is, the washing is part of the protective effect of a cloth mask,” MacIntyre says. She recommends a daily wash in water at 60° to 90° Celsius, far hotter than anyone could stand to hand-wash. Shrinkage from hot water also tightens up pores in the mask, keeping the virus from slipping through easily.
Health care workers should also wear protective goggles to prevent rare cases of infection through the eye, MacIntyre says. But determining whether people going about their daily lives need goggles, face shields or other eye protection in addition to masks is a tricky bit of calculus, she says. “You have to look at community transmission rates. You have to look at where you’re actually going. Are you just going for a walk outside or are you going to a doctor’s surgery and are going to be sitting in an unventilated waiting room for two hours?”
The best most people can do is to take all the precautions they can, including avoiding large gatherings — especially indoors — wearing masks and keeping distance from people they don’t live with.
Fine-tuning lockdowns Early in the pandemic, lockdowns and social distancing measures (of varying severity) enacted in many countries largely worked. Staying at home starved the virus of transmission opportunities, preventing over 500 million infections in six hard-hit countries, according to some experts (SN: 6/9/20).
Circumstances are different now. “I don’t think we’ll lock down at that scale again,” says Michael Osterholm, an epidemiologist at the University of Minnesota in Minneapolis and a member of Biden’s task force. Now that scientists have a better understanding of transmission, blanket lockdowns may not be needed. Instead, restrictions could focus on crowded, poorly ventilated spaces like restaurants and bars.
If cases continue to grow exponentially, however, stricter lockdowns may be the only tool left to prevent hospitals from being overwhelmed. But such measures are increasingly less palatable to many Americans, Osterholm says. “What the public will accept is key. If they won’t comply, it doesn’t really matter what you recommend or how you recommend it.”
Limits of lockdowns Stay-at-home orders also don’t stop transmission within a household, where experts are learning that the virus can rapidly spread. In a sample of 101 homes with a positive coronavirus test, 53 percent of other people living in those homes became quickly infected, researchers reported in the Nov. 6 Morbidity and Mortality Weekly Report.
“We know that it’s really gatherings in close contact indoors that are riskiest,” says Alison Hill, an epidemiologist at Johns Hopkins University. “There’s no reason why if you’re in your own house or among family or friends to think that the disease can’t spread.” Isolating infected members of a household, wearing masks and improving ventilation can limit household transmission, she says.
And not everyone can stay home, which has contributed to inequities in who is getting sick in this pandemic.
In the United States, residents of poorer neighborhoods, often home to racial and ethnic minorities disproportionately affected by COVID-19 (SN:4/10/20), were less likely to stay at home during the early months of the pandemic than residents of richer neighborhoods. Cell phone mobility data suggest that this difference stems from work-related demands, according to a study published November 3 in Nature Human Behavior. Residents of the highest-income neighborhoods reduced days at work outside the home by 13.7 percent, compared with 6.6 percent for residents of lower-income neighborhoods, Jonathan Jay, a public health researcher at Boston University, and colleagues found.
Many residents of lower-income neighborhoods work jobs that can’t be done from home. But when there was a choice, people in these neighborhoods did limit their activities, Jay says. The data showed that people of all income groups reduced outings unrelated to work at roughly similar levels.
Policies like restricting evictions so people don’t fear losing their home if they miss work, expanding unemployment insurance and mandating paid sick leave could help these residents physically distance, Jay says.
Test and trace Lockdowns by themselves will not end the pandemic. They are only supposed to be temporary measures that buy time for local and state health departments to beef up other infection-control strategies. Crucial among these are testing and contact tracing, a tried-and-true public health intervention whereby contacts of positive cases are quickly identified and instructed to quarantine (SN: 4/29/20).
“Contact tracing is really key when you have a disease that’s as fast-spreading as COVID-19,” because it breaks crucial chains of transmission, says Martial Ndeffo, an infectious diseases researcher at Texas A&M University in College Station.
Contact tracing and isolation is most powerful when cases are identified early in the course of infection, their contacts are traced and informed of their exposure quickly, and those contacts comply with requests to quarantine. Such a system requires broadly available testing and lots of contact tracers to do the detective work. Otherwise, even with relatively small caseloads, contact tracing systems can’t keep up with a growing epidemic. At this point, most of the United States can’t keep up. In October, only three states and the District of Columbia had enough full-time contact tracers to deal with current caseloads, according to a survey conducted by NPR and the Johns Hopkins Center for Health Security. And as cases climb, even well-staffed systems could be overwhelmed.
“Given the number of cases in the U.S., it is unrealistic to think that most states have the resources and available staff to raise the army of contact tracers needed,” Ndeffo says. Biden’s COVID-19 response plan includes efforts to “mobilize at least 100,000 Americans across the country” to boost the contact tracing effort. Currently, there are just over 50,000 contact tracers nationwide.
Robust contact tracing systems work only if people comply with public health officials and share their contact history or quarantine if necessary. Yet only 58 percent of Americans would be likely to speak with a public health official who contacted them by phone or text message about the coronavirus outbreak, according to a Pew Research survey released October 30. “A substantial number of people do not comply with or provide adequate information needed for contact tracing to be effective,” Ndeffo says. Clearer and more consistent public health messaging could improve these numbers.
Time is of the essence It’s important to act quickly to introduce social distancing measures when case counts begin to surge, as they are now in the United States and Europe, Shaman says, because outbreaks grow at exponential rates. “Exponential growth leads to a tsunami-like effect; it gets worse the longer you wait on it.”
He and colleagues simulated what would have happened had states done exactly what they did at the beginning of the U.S. epidemic in March, only earlier. Enacting social distancing and stay-at-home orders on March 1 instead of March 8 would have headed off about 600,000 confirmed cases and 32,000 deaths. Acting two weeks earlier would have avoided more than 1 million cases and about 60,000 deaths nationwide, Shaman and colleagues reported November 6 in Science Advances.
No one can turn back the clock. But countries including Vietnam, Taiwan, Singapore, New Zealand and Australia have shown that acting aggressively can curb the spread of the virus. “Going forward, the longer you delay in acting on this virus the more damage it does,” both to people who are infected and to the economy, Shaman says.
For instance, at the end of September, 89 counties in Tennessee eased or removed social distancing restrictions. But as COVID-19 cases rose, traffic to bars and restaurants decreased, researchers from Vanderbilt University in Nashville report. Cell phone mobility data as of October 21 suggest that business dropped once restrictions were lifted and was 24 percent below where it was during the same time in 2019. Those findings suggest that infection rates, not restrictions, have a bigger effect on people’s choices, the researchers conclude.
“If you don’t control the virus,” Shaman says, “you’re not going to have an economy.”
A long-sought “holy grail” in cryptography is poised to change the way we protect sensitive information.
Today’s standard encryption schemes take an all-or-nothing approach. Once scrambled, your data become inaccessible to anyone without the secret key.
This has allowed for secure e-mail communication, the proliferation of online transactions and digital signatures. It allows tax and medical records with sensitive personal information to be passed more safely across the internet. But if you give someone the secret key to access any of the data, all of the data become vulnerable.
What if instead you could assign specific people access to do very specific things with your data? Someone could get the information they need (the info you want them to have) without unlocking all of the original data. Bank details, credit card numbers, account passwords – all would remain hidden. That wholly different approach could also allow Netflix to make show recommendations without seeing your full viewing history, for example. Google could sort your e-mails without knowing what’s in them. And medical researchers could analyze data to identify risk factors for a disease without accessing any individual’s health information.
This and other cryptographic wonders now appear possible through a master tool called indistinguishability obfuscation.
“It’s a new tool – a very powerful tool,” says cryptographer Huijia (Rachel) Lin of the University of Washington in Seattle who showed with colleagues in 2020 how to construct the tool. “Once you have this superstrong power, then a lot of the other tasks are either special cases of it, or you can easily use this to realize [those tasks].”
Vinod Vaikuntanathan, a computer scientist at MIT who has worked with Lin on previous research, compares indistinguishability obfuscation, or iO, to a grand theory in physics that would unite gravity and quantum mechanics. “iO gives you a way to do a grand unification of cryptography in the sense that you can explain much of what cryptography does in a very simple way.” Standout research Indistinguishability obfuscation is a form of program obfuscation, an approach that seeks to hide the inner workings of a computer program, not just the message or data itself. Though proposed in 1976 in a paper that set the foundation for modern cryptography, program obfuscation proved difficult to achieve. For many years, people thought it might not be possible.
And in 2001, researchers showed that complete program obfuscation — called black-box obfuscation, in which input and output data are known but nothing else about a program can be discovered — is impossible. Yet indistinguishability obfuscation, proposed at the same time and shown to be incredibly powerful, doesn’t demand that everything about a program remain hidden. It instead deals with two programs that perform the same function. If the inner workings of those two programs can be hidden enough that the two can’t be distinguished from each other, indistinguishability obfuscation has been achieved. By hiding the secret key within the program itself, iO enables the delegation of specific data and data tasks to specific people.
Still, proposal after proposal for making iO work proved breakable. Researchers couldn’t figure out how to keep it safe from an adversary’s attacks. Lin says the approaches being used didn’t appeal to her. Researchers were leaning on what appeared to be “good enough” ways of getting at the problem that weren’t backed by rigorous mathematical proofs.
Lin instead wanted to break the problem down so she could understand each component and how they worked together. She wanted to approach the problem like a clock, with gears and nuts and bolts, instead of tangled like “a bowl of spaghetti.”
Through this strategy, Lin, along with Amit Sahai of UCLA and Aayush Jain, a Ph.D. student at UCLA at the time, demonstrated that iO is achievable. It would be secure based on standard assumptions in the field, the team proved, renewing hope in the tool.
“Of course, [Huijia] is brilliant,” Vaikuntanathan says, adding that her persistence is what really sets her apart. “It takes some guts to continue with an approach when essentially all the rest of the world thinks that it is not going to work.”
Backstory Lin says she didn’t grow up with computers or fall in love with computer programming at an early age. As a student, she was interested in physics and strived to be good at everything. She started with computer science in college; a class in cryptography as a Ph.D. student at Cornell University “was really mind-opening,” she says. Her introduction to what are known as zero-knowledge proofs stands out in her memory.
A zero-knowledge proof says that a person can convince someone else that they know a secret without revealing the secret or any details about it. Say, for example, you knew that a number was the product of two prime numbers. Can you convince someone that fact is true without revealing what the primes are? How to prove that such a task is possible fascinated Lin. Cryptography includes a lot of these seeming paradoxes that prove to be possible. Indistinguishability obfuscation is yet another example – and Lin works on others, including secure multiparty computation, which allows a computer task to run across multiple people’s data without any person having to reveal their data to anyone in the group, or to a third party.
“I’m very attracted to these magical concepts,” Lin says. “The fun of it is to make this concept come to realization.”
Indistinguishability obfuscation is still far from real-world implementation. But Vaikuntanathan says it’s not unusual for first constructions of what will become important approaches to be impractical at first. “Wait for a decade,” he says.
Environmental engineer Smruthi Karthikeyan had spent just a couple of days working in her new lab at the University of California, San Diego when the state instituted its first coronavirus lockdown in March 2020.
She’d been brought on as a postdoc by biologist Rob Knight to develop new techniques for studying how microbes in complex ecosystems shape human health and vice versa. The COVID-19 pandemic quickly put a new spin on that mission.
Soon, the lab pivoted to support the coronavirus response. Infections were outpacing testing capacity in San Diego County, Karthikeyan says. Meanwhile, the university wanted to keep the campus open for its 10,000 students still living on campus and 25,000 workers. There had to be a way to monitor infections without requiring thousands of people to get tested all the time, Karthikeyan and colleagues thought.
Public health researchers had previously tested wastewater for pathogens as a way to spy on the movements of infectious agents in communities. Viruses, bacteria and parasites can show up in stool before people exhibit symptoms, giving clues to a coming outbreak. But no one had implemented such a system to track a respiratory virus before, and never at a scale of tens of thousands of people.
Karthikeyan was up for the challenge.
Bold idea The wastewater monitoring system that Karthikeyan and colleagues developed and implemented at UC San Diego, reported July 7 in Nature, processes upward of 200 samples per day. Previous methods could process a maximum of eight samples, she says. What’s more, the system has identified newly spreading coronavirus variants up to two weeks earlier than clinical testing and accurately forecasted the mix of variants infecting students and staff.
That has given school officials more time to take action to keep infection rates low. During the study period from November 2020 to September 2021, the proportion of clinical tests that were positive was less than one percent, Karthikeyan says, dramatically lower than rates in the surrounding area and many other college campuses at the time. Among the key players in the team’s monitoring system are 131 robots that collect wastewater samples throughout each day from 360 university buildings. Back at the lab, the samples are screened for viral RNA and results are fed into a publicly available online dashboard created as part of the project.
Karthikeyan’s team isn’t the only one using human waste to get a jump on COVID-19. But the scale of the monitoring “is a bit unprecedented,” says Ameet Pinto, an environmental engineer at Georgia Tech in Atlanta. During the study period, Karthikeyan and colleagues processed a total of nearly 20,000 samples. “That’s amazing,” he says.
A positive result triggers a campus-wide notification via smartphone app. For dorms, anyone who lives in the building is mandated to get tested for COVID-19, while anyone who may have recently been in the building is strongly encouraged to get tested.
To increase access to tests, the team swapped candy in vending machines for at-home test kits and installed test drop boxes in the buildings. Karthikeyan’s team processes the tests and sends results within a day.
Anyone testing positive for the coronavirus is moved to a designated isolation dorm or instructed to isolate at home if they live off campus. If the coronavirus shows up in the next day’s wastewater test, the building’s remaining occupants will receive a notification to test again.
To figure out which variants are causing infections at the university, Karthikeyan’s team built a freely available computational tool called Freyja. It uses a library of genetic markers to identify the relative abundances of well-known and emerging variants in the wastewater. Freyja detected the emerging delta variant on campus 14 days before clinical tests did, Karthikeyan and colleagues report.
Growing the effort Based on success at the university, San Diego County officials asked the researchers to test a modified version of the system at the Point Loma Wastewater Treatment Plant, which serves more than 2.2 million residents, and at 17 public schools. Elementary school students got to name the robots, dubbing the machines Sir-Poops-a-Lot, Harry Botter and the Rancid Water, and other silly monikers, Karthikeyan said with a chuckle.
On the county level, the system detected the emergence of the omicron variant 11 days before clinical testing, the team reports in the same study in Nature. A detailed analysis of the public school data hasn’t yet been published.
Karthikeyan and colleagues’ methods have been adapted by researchers at the state, national and international levels. For instance, the U.S. Centers for Disease Control and Prevention and the Food and Drug Administration use Freyja to track variants in wastewater across the country.
The system is now being used to monitor monkeypox, and the team is working on how it can detect other pathogens that may be spreading unnoticed. That work has the potential to have a huge impact on wastewater epidemiology, Pinto says.
Karthikeyan will launch her own lab at Caltech in 2023, where she plans to adapt these tools for monitoring groundwater. Communities of microbes that live there can serve as sentinels, flagging disturbances from pollution, climate change and more, she says. “My whole thing is to look at a much larger system from a very tiny lens.”
Some of the earliest stars yet seen are now coming to light in one of the first images from the James Webb Space Telescope.
Formed roughly 800 million years after the Big Bang, the stars live in dense groups called globular clusters and surround a distant galaxy dubbed the Sparkler, astronomers report in the Oct. 1 Astrophysical Journal Letters. Globular clusters often host some of the oldest stars in contemporary galaxies such as our own, but it’s hard to tell their exact age. The new finding could help researchers pinpoint when such clusters began to form.
Compared to a galaxy, globular clusters are tiny, which makes them hard to see from across the universe. But this time, a gargantuan natural lens in space helped. The Sparkler is one of thousands of galaxies that lie far behind a massive, much closer galaxy cluster called SMACS 0723, which was the subject of the first publicly released science image from the James Webb Space Telescope, or JWST (SN: 7/11/22). The cluster distorts spacetime such that the light from the more distant galaxies behind it is magnified.
For all those remote galaxies, that extra magnification brings out details that have never been seen before. One elongated galaxy surrounded by yellowish blobs got the attention of astronomer Lamiya Mowla and her colleagues.
“When we first saw it, we noticed all those little dots around it that we called ‘the sparkles,’” says Mowla, of the University of Toronto. The team wondered if the sparkles could be globular clusters, close-knit families of stars that are thought to have been born together and stay close to each other throughout their lives (SN: 10/15/20).
“The outstanding question that there still is, is how were the globular clusters themselves born?” Mowla says. Were they born at “cosmic noon,” 10 billion years ago, when star formation throughout the universe peaked? Or did they form 13 billion years ago at “cosmic dawn,” when stars were first able to form at all (SN: 3/4/22)?
Light from the Sparkler takes about 9 billion years to reach Earth, so if the sparkles are globular clusters that shone that long ago, they might help astronomers answer that question. Mowla and her colleagues used data from JWST to analyze the wavelengths of light coming from the sparkles. Some of them appear to be forming stars at the time when their light left the clusters. But some had formed all their stars long before.
“When we see them, the stars are already about 4 billion years old,” says astrophysicist Kartheik Iyer, also of the University of Toronto.
That means the oldest stars in the sparkles could have formed roughly 13 billion years ago. Since the universe is 13.8 billion years old, “there’s only a short amount of time after the Big Bang when these could have formed,” he says.
In other words, these clusters were born at dawn, not at noon.
Studying more globular clusters around ancient galaxies could help determine if such clusters are common or rare early on in the universe’s history. They could also help unravel galaxies’ formation histories, say Mowla and Iyer. Their team has proposed observations to be made in JWST’s first year that could do just that.
Being able to pick out tiny structures like globular clusters from so far away was almost impossible before JWST, says astronomer Adélaïde Claeyssens of Stockholm University. She was not involved in the new work but led a similar study earlier this year of multiple galaxies magnified by the SMACS 0723 cluster.
“It’s the first time we showed that, with James Webb, we will observe a lot of these type of galaxies with really tiny structures,” Claeyssens says. “James Webb will be a game changer for this field.”
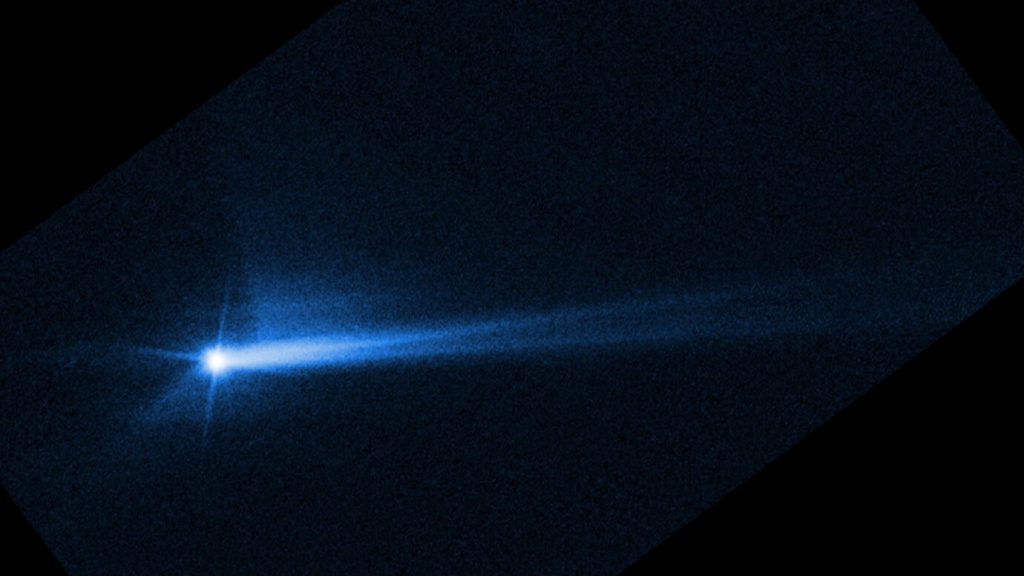
It worked! Humanity has, for the first time, purposely moved a celestial object.
As a test of a potential asteroid-deflection scheme, NASA’s DART spacecraft shortened the orbit of asteroid Dimorphos by 32 minutes — a far greater change than astronomers expected.
The Double Asteroid Redirection Test, or DART, rammed into the tiny asteroid at about 22,500 kilometers per hour on September 26 (SN: 9/26/22). The goal was to move Dimorphos slightly closer to the larger asteroid it orbits, Didymos.
Neither Dimorphos nor Didymos pose any threat to Earth. DART’s mission was to help scientists figure out if a similar impact could nudge a potentially hazardous asteroid out of harm’s way before it hits our planet.
The experiment was a smashing success. Before the impact, Dimorphos orbited Didymos every 11 hours and 55 minutes. After, the orbit was 11 hours and 23 minutes, NASA announced October 11 in a news briefing. “For the first time ever, humanity has changed the orbit of a planetary body,” said NASA planetary science division director Lori Glaze.
Four telescopes in Chile and South Africa observed the asteroids every night after the impact. The telescopes can’t see the asteroids separately, but they can detect periodic changes in brightness as the asteroids eclipse each other. All four telescopes saw eclipses consistent with an 11-hour, 23-minute orbit. The result was confirmed by two planetary radar facilities, which bounced radio waves off the asteroids to measure their orbits directly, said Nancy Chabot, a planetary scientist at Johns Hopkins Applied Physics Laboratory in Laurel, Md.
The minimum change for the DART team to declare success was 73 seconds — a hurdle the mission overshot by more than 30 minutes. The team thinks the spectacular plume of debris that the impactor kicked up gave the mission extra oomph. The impact itself gave some momentum to the asteroid, but the debris flying off in the other direction pushed it even more — like a temporary rocket engine.
“This is a very exciting and promising result for planetary defense,” Chabot said. But the change in orbital period was just 4 percent. “It just gave it a small nudge,” she said. So knowing an asteroid is coming is crucial to future success. For something similar to work on an asteroid headed for Earth, “you’d want to do it years in advance,” Chabot said. An upcoming space telescope called Near-Earth Object Surveyor is one of many projects intended to give that early warning.
A genetic variant that appears to have boosted medieval Europeans’ ability to survive the Black Death centuries ago may contribute — albeit in a small way — to an inflammatory disease afflicting people today.
Researchers used DNA collected from centuries-old remains to discern the fingerprints that bubonic plague during the Black Death left on Europeans’ immune systems. This devastating wave of disease tended to spare those who possessed a variant of a gene known as ERAP2, causing it to become more common, researchers report October 19 in Nature. That variant is already known to scientists for slightly increasing the odds of developing Crohn’s disease, in which errant inflammation harms the digestive system.
The results show “how these studies on ancient DNA can help actually understand diseases even now,” says Mihai Netea, an infectious diseases specialist at Radboud University Medical Center in Nijmegen, Netherlands, who was not involved with the study. “And the trade-off is also very clear.”
Caused by the bacterium Yersinia pestis, bubonic plague once killed 60 percent of those infected (SN: 6/15/22). In the ancient world, it caused successive waves of misery, the most devastating of which was the Black Death, often dated from 1346 to 1350, an episode thought to have wiped out at least 25 million people — about a third or more of the European population.
By sparing individuals whose immune systems bear certain traits, pathogens such as Y. pestis have shaped the evolution of the human immune system. Studies are teasing out the ways the massive winnowing of the plague altered Europeans’ immune-related genetics.
In this most recent study, population geneticist Luis Barreiro of the University of Chicago and colleagues collected samples containing DNA from the remains of 516 people in London and Denmark who died between 1000 and 1800, including those buried during the Black Death. The researchers examined stretches of DNA for immune-related genes and areas associated with autoimmune and inflammatory diseases. Within those regions, the researchers identified four locations on chromosomes where they saw strong evidence of genetic changes that appeared to have been driven by the Black Death. In follow-up work, one change stood out: an increase in the frequency of a variant of ERAP2. When infected with Y. pestis, immune cells from people with this version of ERAP2 more effectively killed the bacteria than cells lacking the variant. Studies of modern populations have linked that same variant to Crohn’s disease.
While the researchers calculate that the ERAP2 variant improved the odds of surviving the Black Death by as much as 40 percent, it only slightly increases the risk for Crohn’s disease. For complex disorders like Crohn’s, “you require probably hundreds, sometimes thousands of genetic variants to actually increase your risk in a significant manner,” Barreiro says.
For some time now, researchers in the field have theorized that adaptations that helped our ancestors fortify their immune systems against infectious diseases can contribute to excessive, damaging immune activity. Earlier studies of plague offer support for this idea. A genetic analysis seeking traces of historical disease in modern Europeans and a study of DNA from the remains of 16th century German plague victims both turned up what appear to be protective changes against the plague that, like the ERAP2 variant, are linked with inflammatory and autoimmune conditions.
Likewise, this latest discovery suggests that genetic changes that have amped up the human immune response in the past, empowering it to better fight off ancient infections, can come at a cost. “If you turn the heat too much, that leads to disease,” Barreiro says.